The Family Planning Estimation Tool (FPET) was designed to produce annual estimates of mCPR, CPR, unmet need, and demand satisfied by modern methods using statistical modelling that incorporates all available data. FPET is unique in that it considers survey data, service statistics (where determined to be of adequate quality), and regional and global historical patterns of change to produce annual estimates beyond the last survey and into the future.
The model was adapted from one used by the United Nations Population Division for estimating family planning trends for all countries in the world. The adaptation was prepared by Jin Rou New and Leontine Alkema1. The FPET model is an online tool that can be run for one country at a time and allows users to input their own data.
Estimates for mCPR and unmet need are usually taken from population-based surveys, such as the DHS. However, because most countries do not conduct such surveys annually (with some exceptions, including countries with PMA2020), many countries must wait five or more years for updated data. Even when recent survey data are available, results from surveys do not always tell a clear story about current progress, or, help to project future trends.
The graph below shows trend data for mCPR for married women from four different types of surveys in Nigeria. As this graph shows, comparing different types of surveys can sometimes provide misleading information. Each type of survey has its own trend that sits at a slightly different level of mCPR. For example, comparing the 2008 DHS to the 2011 MICS survey would give the impression that mCPR has increased, which the arrival of the 2013 DHS would have contradicted. However, when you look at all of the trends together, they show the same thing, stagnation.
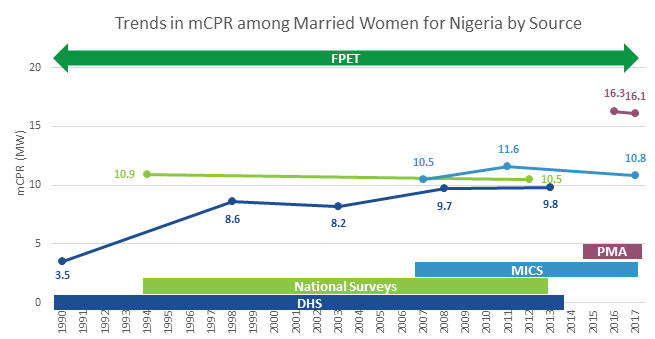
FPET allows for all of the various types of survey data to be integrated into the estimates and fits a line that pulls from all of the trends. This utilizes the strength of multiple data points and minimizes the risk of comparing different surveys.
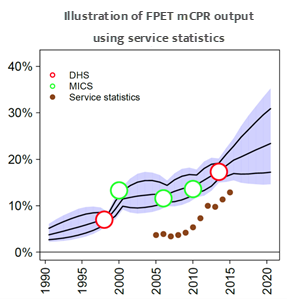
In addition to surveys, routine family planning service statistics are collected and reported on an annual basis in most countries, but tend to be under-utilized in planning and decision-making. While such data cannot provide “stand-alone” estimates of modern contraceptive prevalence, it can be used to help inform a country's progress. FPET allows the user to incorporate their own service statistic data into the estimation process, which can increase the accuracy of the estimates after the last survey.
Although contraceptive use estimated from service statistics data may not be correct with regard to level, service statistics may be used to measure the trends in mCPR over a 3 to 5-year period since the last DHS, thus improving the accuracy of the most recent mCPR estimates
Track20 has developed the Estimated Modern Use (EMU) Tool to help countries review their service statistics, and produce EMU estimates that can be fed into FPET if minimum quality criteria are met.
FPET is a Bayesian hierarchical model, meaning that it estimates the likelihood of a given future result based on global knowledge of how countries’ contraceptive prevalence rates have historically transitioned from low to high, and is informed by data at multiple levels (country, sub-regional, regional, global). The model fits a logistic growth curve to CPR data for all methods to determine the long-term trend in contraceptive use and adds a time-series model with autocorrelation to capture country-specific deviations around the long-term trend.
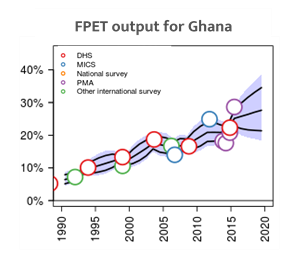
FPET not only determines the most likely trends in family planning outcomes, but also estimates an uncertainty range around the trends so that each estimate contains a median estimate as well as a 95% confidence range, as shown in the figure above for mCPR.
When fitting models, FPET distinguishes between different types of data (e.g., DHS versus other national surveys), and uses standard errors to determine the pull of the curve, allowing greater weight to sources of data with lower estimated error variance (in the model, DHS have the lowest error variance).
The long-term trend is characterized by an asymptote (where the trend levels off), as well as the pace and timing of the increase. These three parameters are estimated from national data and informed by regional patterns.
A second model splits total contraceptive use into modern and traditional methods. A third model fits trends in unmet need. Related outcomes, such as total demand for family planning, are calculated based on the different model fits
Estimates for previous years were based on the 'level' model which estimates historical trends by fitting curves to data on the level of mCPR. This approach smooths fluctuations from survey to survey and identifies the long- term trend, but it is relatively insensitive to short-term recent changes. Since we want to know whether trends have changed for the better since the start of FP2020, the ‘level’ model may under-estimate true progress.
Starting in 2017, FPET was updated to a 'rate' model, which fits trend curves to rates of change in mCPR rather than levels of mCPR. While this approach risks giving too much weight to recent, short term changes, it should be better at identifying recent changes that are the result of real progress. The effect of this change on current year estimates is small, but projections to 2020 should be more sensitive to recent progress.
FPET can be accessed at: http://fpet.track20.org