Excerpt from FP2020 Commitment to Action 2014-15: Measurement Annex
FP2020's goal of empowering 120 million additional women and girls to use modern contraception must be attained in a way that is inclusive of all women, including young people. The analyses presented below gives a snapshot of contraceptive use and non-use among married and unmarried sexually active young women. It is clear that patterns of use among young women vary greatly by country; some countries seem to have much more equitable use and knowledge of family planning by both married and unmarried young women, whereas in other countries, large discrepancies exist.
While we don't have a reliable estimate of unmet need among all youth (married and unmarried), it is clear that the need for contraception is pervasive. Comprehensive sexuality education can ensure that young people have the knowledge and tools to make informed decisions about using contraception, preventing unwanted pregnancies, and protecting themselves from sexually transmitted infections, including HIV. In some countries, policies restrict young people's fundamental right to sexual and reproductive health information, services, and supplies. Even when policy barriers have been removed, stigma and provider bias often prevent young people from seeking or receiving information and services.
The following analysis, adapted from the FP2020 Commitment to Action 2014-15 Measurement Annex, will look at the available evidence regarding contraceptive use, knowledge, and attitudes among both unmarried and married young women age 15 to 24.
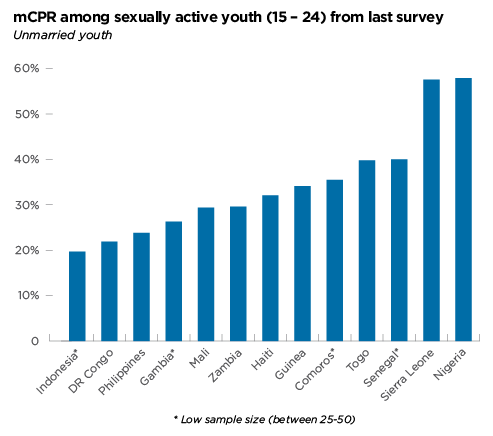
Are unmarried youth using modern contraception? Modern contraceptive prevalence among unmarried women is measured among those who are sexually active - defined as women who reported having had sex in the 4 weeks prior to the survey. This analysis looks exclusively at sexually active unmarried young women, aged 15 - 24.
Of the 41 countries with data collected since the time of the London Summit on Family Planning, 13 countries have usable data on sexually active unmarried youth.[1] The figure below shows that in these 13 countries, levels of contraceptive use among this group vary widely, from just under 20% in Indonesia, to nearly 60% in Sierra Leone and Nigeria.
Current levels of use are important, but it is also useful to see how contraceptive use among this group is changing over time. In the chart below, countries have been categorized based on changes between the last two surveys in mCPR for sexually active unmarried young women, and how these changes compare to changes in mCPR among married young women.[2]
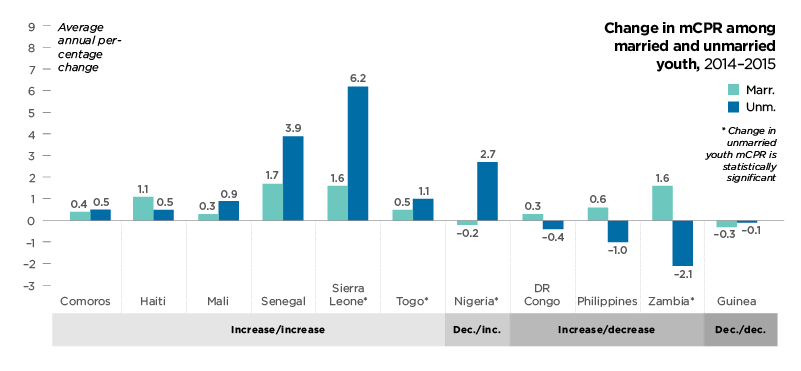
Countries fell into 1 of 4 groups: mCPR increase in both married and unmarried sexually active youth; mCPR decrease in both populations; and the opposites of both groups. In the majority of countries, increases in mCPR among both unmarried and married young women were observed. Of these countries, Sierra Leone is notable because mCPR for unmarried young women grew nearly 4 times faster than mCPR among married young women.
Four countries experienced declines in mCPR among unmarried young women, and in most of these countries this decline happened despite increases in mCPR among married young women. Nigeria also stands out in this analysis; while there was no increase in mCPR for married young women, a very large increase among unmarried young women was seen. The asterisks in the table below note changes in unmarried mCPR that are statistically significant.
Does marriage lead to improved access to contraception for young women? It is sometimes assumed that once women are married, barriers to contraception will be removed. However, in some places, young married women still face barriers to contraceptive use.
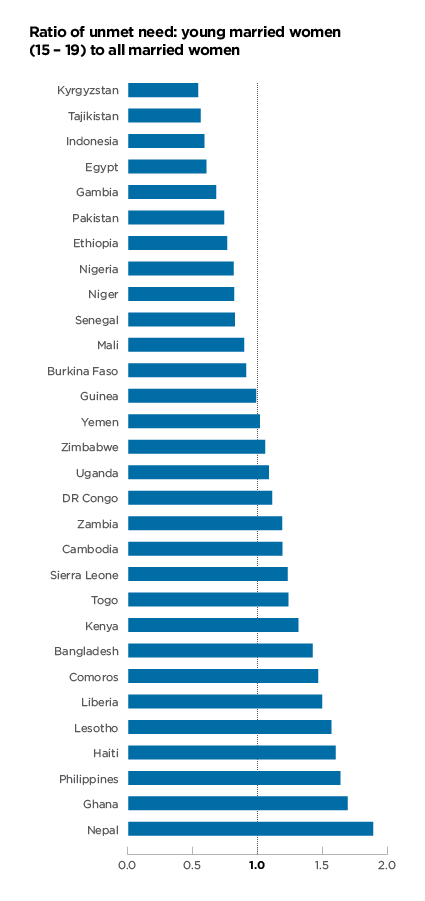
One way to look at this is by examining the ratio of unmet need for contraception among young married women (15-19) compared to all married women. A ratio of one would mean their levels of unmet need are identical, anything under one means young married women have lower unmet need, and anything over one means young married women have higher unmet need.
As can be seen below, in more than half of the countries with recent data, unmet need is higher among young married women (orange bars). In Nepal, the unmet need among married 15-19 year olds is nearly twice that of the total unmet need for all married women of reproductive age.
There are many complex factors that drive these different patterns in unmet need among young unmarried women. To fully understand why countries have a low or high ratio of unmet need among young married women compared to all married women would require further study at the country level regarding the cultural context and other drivers of these issues. However, we can begin to analyze some of the underlying dynamics.
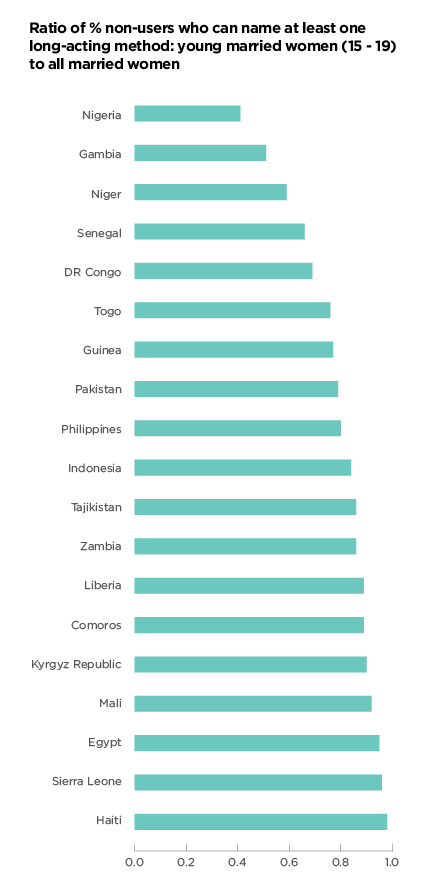
One potential driver of this pattern could be discrepancies in knowledge of modern contraception. Overall, knowledge of modern methods is fairly similar across all age groups. However, when looking at knowledge of at least one long-acting contraceptive method (IUD or Implant), large discrepancies can be seen[3]. In fact, in all countries included, a lower proportion of non-users aged 15-19 could name at least one long-activing method, then across all married women.
This pattern does not match to the ratios of unmet need, meaning it cannot explain all of the difference in unmet need between young married women and married women as a whole. However, it suggests that in some countries, more work is needed to ensure that all married women have the same access to information about contraceptives.
What similarities and differences are there between married and unmarried sexually active youth? Understanding differences in the reasons for not using contraception and exposure to family planning health care providers may help to explain some of the differences in levels of use between these two groups. This analysis includes 6 countries that have had a recent DHS survey with a sufficient number of unmarried sexually active women to allow for further analysis.
Do the reasons for non-use of contraception vary for married and unmarried sexually active youth? To answer this, responses on four selected questions about reasons for non-use are shown below. Young women were able to respond 'yes' to more than one reason, meaning the same women may be included under different reasons. As might be expected, we see that infrequent sex is more commonly cited as a reason for non-use among unmarried sexually active than married young women (28.2% v 8.9% on average). And similarly that many more married young women cited breastfeeding as a reason for non-use (40.1% v 3.1% on average).
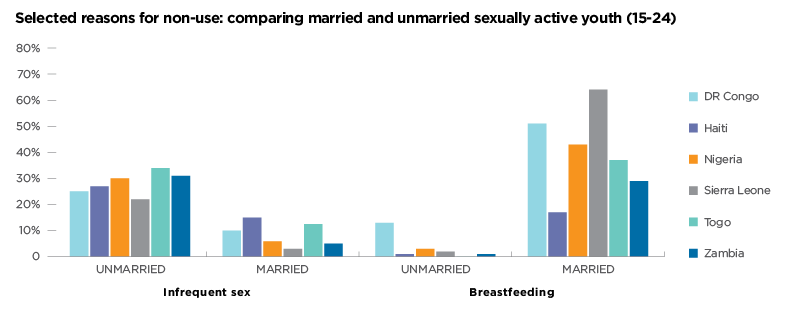

For some reasons for non-use we see less distinction between responses from married an unmarried young women. Non-use due to fear of side effects varies largely across countries, and between married and unmarried young women. Non-use due to lack of access or services too far is generally low, but, some differences between married and unmarried women can be seen. This is especially true in Sierra Leone where 4 times the % of unmarried young women cited this as a reason for non-use than married young women.
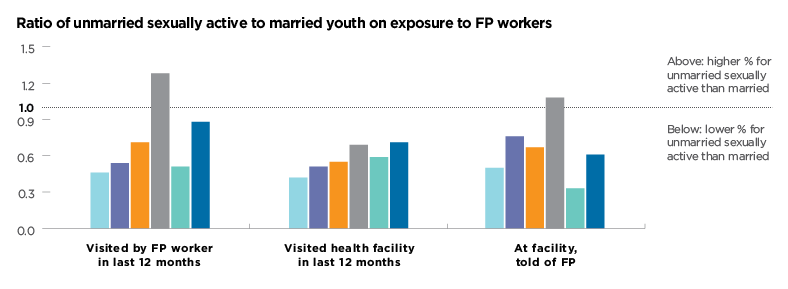
Do married and unmarried sexually active young women have the same access to family planning service providers? To answer this, three questions related to interactions with service providers are examined in the figure below. For both unmarried sexually active and married young women, visits by family planning health workers are fairly low (10.3% and 11.8% on average).
More variation is seen in terms of visiting health facilities (31.3% and 53.1% on average), and for those visiting facilities being told about family planning (31.6% and 44.8% on average). Comparing the ratio between married and sexually active unmarried youth highlights gaps in exposure to family planning services. Aside from Sierra Leone, in all of the other five countries, exposure to family planning information and services is considerably lower for unmarried sexually active youth than married youth, regardless of the venue in which this exposure happens (family planning worker or at a facility).
To better understand what is driving these trends, the country context and more country specific knowledge is needed. For example, what can be learned from countries like Nigeria and Sierra Leone who have seen large increases in modern contraceptive use by unmarried sexually active young women? And, what can be learned from countries like Haiti and Egypt, who have been able to ensure that young married women have the same levels of contraceptive knowledge as their older married counterparts?
[1] The following countries collected data on unmarried youth, but had to be excluded from the analysis for the reasons noted: DHS surveys in Cambodia, Niger and Tajikistan were excluded from the analysis due to too few sexually active unmarried women in the sample. DHS surveys in Ghana, Kenya and Lesotho were excluded because at the time of writing only the Key Indicator Reports were available for these countries, which do not provide data on unmarried sexually active contraceptive use by age. PMA2020 surveys were excluded due to an inconsistency in the calculation of recent sexual activity - this has been corrected, and PMA2020 data will be included in the next youth analysis where sample sizes permit.
[2] Note: Gambia and Indonesia are excluded from this analysis because no prior estimate of sexually active unmarried mCPR was available for comparison.
[3] Note: some countries are excluded from this analysis because their full data sets were not available.